A
Stepwise (Cost-Sensitive)
Start broad, then escalate as needed.
- Start with ELISA (serum/plasma).
- If positive → consider trending/monitoring.
- If negative but symptoms persist → escalate to Mass Spectrometry.
A methodology-based guide to ELISA, Mass Spectrometry, and Antigen-Release Testing — and why biological compartment determines interpretation.
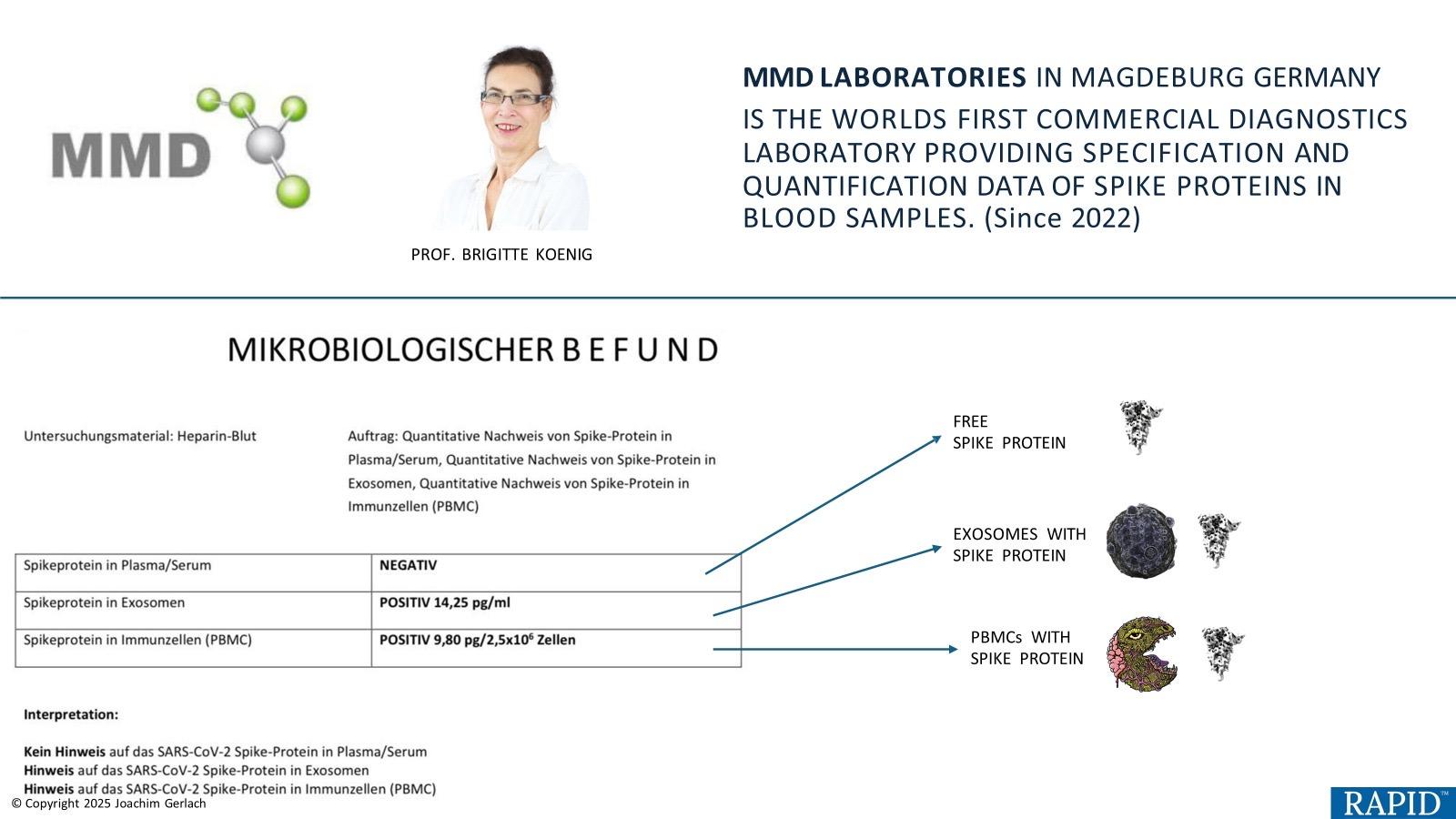
The more useful question is: where is spike located — and what form is it in? Different methods see different compartments, which changes interpretation.
Each method answers a different clinical question: screen, measure, or confirm.
Compartment mapping
A “negative” result can mean different things depending on the compartment tested.
Testing Method
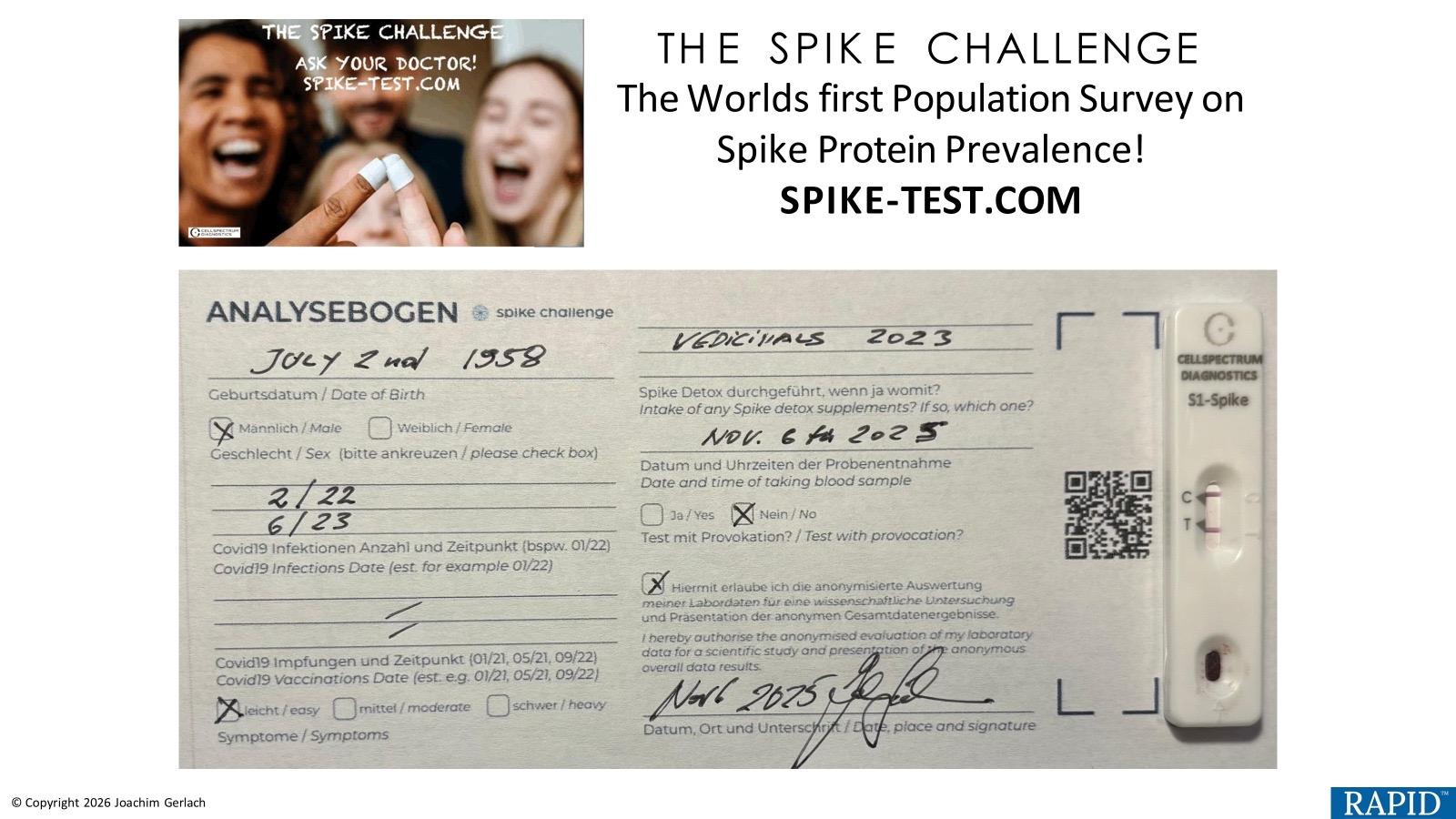
A rapid screening approach designed to answer one question quickly: is there a detectable spike-antigen signal?
Semi-quantitative (band intensity / signal strength), not a precise concentration value.
Treat as a screening signal. Consider confirmation/quantification with ELISA or MS based on clinical complexity.
A negative screen does not necessarily exclude other compartments/forms. If suspicion persists, consider deeper methods (MS) and/or compartment-specific approaches.
Different tests “see” different biological targets and compartments. Antigen-release formats aim to broaden what becomes detectable in a whole-blood workflow, while ELISA depends on antibody-accessible epitopes and MS detects peptide fragments after digestion.
If symptoms are persistent/complex or you need molecular confirmation, step up to MS; if you want a numeric value for accessible circulating antigen, consider ELISA.
Testing Method
A quantitative immunoassay designed to measure antibody-accessible spike antigen — useful for baseline and trend monitoring.
Numeric concentration (assay-dependent ranges), supporting trending and comparison within the same methodology.
You want a quantitative baseline and symptoms are mild-to-moderate, or you need a scalable monitoring tool.
ELISA is negative/equivocal but symptoms persist, or the presentation suggests deeper compartments/forms — consider MS for peptide-level confirmation.
ELISA depends on intact antibody-binding epitopes and on the antigen being in an accessible compartment. Fragmented/modified or intracellular forms may not register without additional prep.
When trending over time, use consistent pre-analytics and the same methodology wherever possible to reduce variability.
Testing Method
A peptide-level approach designed for molecular confirmation: which spike peptides are present, and at what level.
Quantitative peptide detection with sequence-level confirmation (lab/platform dependent).
MS can detect peptide fragments that antibody-based assays may miss when epitopes are altered or fragmented.
Used when the clinical picture is disproportionate, multisystem, or persistent and higher resolution is needed.
ELISA depends on antibody recognition of specific epitopes; MS detects peptides after digestion, enabling confirmation even when spike is fragmented or modified.
A common pathway is ELISA for baseline/monitoring and MS as the escalation method for severity, persistence, or uncertainty.
It is not uncommon for ELISA and Mass Spectrometry results to differ. This does not necessarily indicate error.
Screening, quantification, and peptide-level confirmation are different analytical goals. This comparison summarizes what each method is designed to resolve.
Practical takeaway: analytical resolution increases from screening (Lateral Flow) to quantification (ELISA) to peptide-level confirmation (Mass Spectrometry).
Workflows
Different clinical contexts call for different sequencing. These pathways summarize common decision flows.
Start broad, then escalate as needed.
High-resolution confirmation first.
Fast signal → confirm with lab method.
Core principle
ELISA and Mass Spectrometry are sequential tools in a rational diagnostic funnel.
Used correctly, these tools reduce diagnostic ambiguity, prevent premature closure, and improve clinical confidence.
Educational use: This page summarizes analytical methodologies used in research and monitoring contexts for spike antigen detection. It is intended for educational purposes and does not replace clinical judgment or constitute a diagnostic guideline.